How We Prevent Collapse — and Stay Less-Invasive ARP (a.k.a. socket preservation) is a day-0 protocol performed immediately after extraction to reduce the predictable post-extraction loss of ridge width/height. Typically the socket is gently debrided, grafted (xenograft/allograft/autogenous dentin, etc.), and sealed with a membrane or soft-tissue substitute; implants are placed immediately or delayed depending on anatomy and primary stability. ARP does not stop remodeling, but it attenuates it versus spontaneous healing. Patient’s may want to jump straight to the patient summary or FAQ Watch related video
Why day-0 planning matters
Remodeling is fast, asymmetric, and buccal-dominant. Classic and modern syntheses show width loss outpaces height loss in the first months; thin facial plates are at greatest risk. PubMed+1 Where we actually lose bone (and why). The maxillary facial plate is thin in most patients (≤1 mm at many anterior sites), so loss of PDL-dependent “bundle bone” drives a buccal drift/inward shift of the ridge after extraction. PubMed+1 How much loss if you do nothing. Contemporary overviews report ~2.4–3.1 mm mean width reduction within ~6 months when unmanaged. Wiley Online Library
Your Day-0 Options (right after extraction)
 Big idea: what you choose the day the tooth comes out decides whether you’ll preserve volume now or rebuild it later.
Big idea: what you choose the day the tooth comes out decides whether you’ll preserve volume now or rebuild it later.
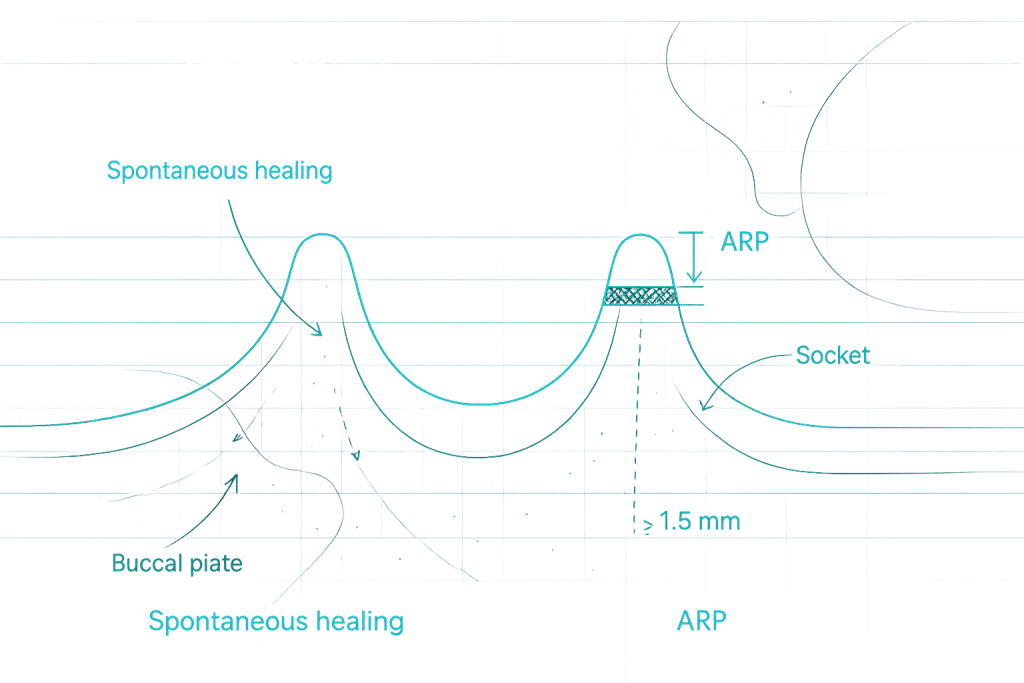
1) Spontaneous healing (no socket preservation)
What it is: gentle extraction; the socket heals with a blood clot only (no graft/membrane). Good when: no implant planned soon; non-aesthetic area; medical/financial constraints. Pros: fastest appointment; lowest immediate cost. Watch-outs: greatest width loss (buccal first) → higher chance of later grafting or sinus lift.
2) Immediate implant
What it is: implant placed the same day as extraction; usually gap grafted to fill the jumping gap. Good when: intact buccal wall; thick phenotype; infection controlled; strong primary stability. Pros: saves time; maintains soft-tissue shape when anatomy is ideal. Watch-outs: still needs palatalized positioning + gap graft to finish with ≥ 1.5–2.0 mm facial bone; not for defective/acute infected sockets.
3) PET (Partial Extraction Therapy / “Socket-Shield”)
What it is: a thin sliver of the buccal root is intentionally retained to support the outer bone and gum; implant placed behind it (usually immediate). Good when: high-aesthetic zone; thin but intact buccal plate; skilled operator. Pros: best at preserving the buccal contour; often fewer grafts later. Watch-outs: technique-sensitive; not for cracked/infected roots or missing buccal plates.
4) ARP (Alveolar Ridge Preservation) + seal → delayed implant
What it is: graft placed in the socket and sealed (membrane or small soft-tissue graft); implant placed later. Good when: thin/defective buccal wall; posterior molars; infection risk; when immediate stability is doubtful. Pros: most predictable volume for a later, simpler implant; helps limit posterior sinus procedures. Watch-outs: two-step timeline; still allows some remodeling (it reduces it—doesn’t stop it). Lets break down ARP slightly more. ARP is a set of socket interventions designed to preserve ridge volume:
- ARP-GM (Graft + Membrane seal) — grafted socket sealed with a collagen/d-PTFE membrane.
- ARP-GS (Graft + Soft-tissue seal) — grafted socket sealed with FGG/CTG or soft-tissue matrix (“socket-seal surgery”).
- ARP-M (Membrane-only) — occlusive membrane (often d-PTFE) used to stabilize the clot/exclude epithelium without graft (select cases).
- ARP-S (Soft-tissue seal-only) — soft-tissue socket seal without graft (rare/selected). ARP-G (Graft-only) — graft placed without a formal seal (least stable; higher exposure risk).
Quick compare (at a glance)
| Option | Primary goal | Best when | Pros | Watch-outs | Typical timeline |
|---|---|---|---|---|---|
| Spontaneous | Let socket heal naturally | No near-term implant; non-esthetic | Fastest, lowest cost | Most width loss → more grafting later | Heal 3–6 mo; graft/implant later if needed |
| Immediate implant | Replace tooth same day | Intact buccal, thick phenotype, high stability | Time-efficient; good soft-tissue if ideal | Must gap graft + position palatal; anatomy-dependent | Surgery day 0; restore after integration |
| PET (Socket-Shield) | Preserve buccal contour | Thin but intact buccal; aesthetic zone | Best contour preservation; fewer big grafts | Technique-sensitive; case-selective | Immediate implant + provisional; standard integration |
| ARP + seal | Preserve ridge for later | Thin/defective buccal; posterior molars | Predictable volume; simpler later implant; fewer sinus lifts | Two stages; some remodeling remains | Extract + ARP day 0 → implant at ~4–6 mo |
| How we decide: CBCT anatomy (buccal plate thickness/defects), soft-tissue phenotype, infection status, aesthetic demands, stability, and your priorities. |
What ARP actually buys you (2024–2025 view)
Systematic reviews and trials consistently show smaller horizontal & vertical changes with ARP versus extraction alone; ARP is risk-reduction, not magic. PMC+1 Posterior maxilla: ARP is associated with less sinus pneumatization and fewer sinus-augmentation procedures later. Wiley Online Library+1 Ballpark CBCT at ~6 months: Several CBCT cohorts report ~0.9–1.2 mm horizontal change with ARP vs ~1.8–2.1 mm without (site-/material-dependent). PMC+1
Materials/adjuncts that minimize downstream invasiveness
Becoming less-invasive with Partial Extraction Therapies (PET)
Socket-Shield/Root-Membrane/submergence maintain buccal PDL blood supply and can improve PES and reduce buccal resorption in selected, technique-sensitive cases; pooled survival ≈98–100% in recent reviews with short- to mid-term follow-up. JPIS+1
Immediate implants — when “immediate” is still minimally invasive
Validated when infection is controlled, primary stability is high, and the buccal plate/phenotype is favorable. Target a thick buccal envelope (≥1–1.5 mm) after placement, 3D-position palato-apically, and gap-graft as needed. PubMed+2OMS Group+2
Timing after ARP: 4–6 months is a practical default
Dimensional stabilization improves between 4–6 months; extending to 12 months generally doesn’t add contour. Histology with mineralized allograft shows similar vital bone at ~3 vs ~6 months, so delaying solely “for more bone” isn’t supported. Georgios A. Kotsakis, DDS, MS.+1
Day-0 decision guide (high-level)
ARP (Socket Preservation): Patient Summary
What it is: A gentle procedure done the same day as your extraction to protect the bone and gum shape. The socket is cleaned, a small bone graft is placed, and the opening is sealed so it heals with better volume. Why it matters: Without planning, the ridge naturally shrinks—especially on the cheek side—in the first few months. ARP means less shrinkage, easier implant placement, and better-looking gums later. It can also reduce the chance of a sinus lift for upper molars. Who benefits most:
- Front teeth / smile zone
- Upper molars What to expect: Local anaesthetic → gentle extraction → graft + seal → stitches. Mild soreness 1–2 days; stitches out in ~1–2 weeks. Implant planning usually at 4–6 months (earlier only when anatomy allows). Risks (uncommon): Membrane/seal exposure, infection, or small residual graft particles on later scans. Smoking and poor hygiene increase risks. Your options at Day-0: Bottom line: Plan the site when the tooth comes out. Smart Day-0 management keeps future treatment simpler, shorter, and less invasive.
Frequently Asked Questions
-
What is ARP?
Alveolar Ridge Preservation is a Day-0 procedure done immediately after tooth removal to reduce natural bone shrinkage. The socket is cleaned, gently grafted, sealed, and allowed to heal. -
Is ARP the same as “socket preservation”
Yes. “Socket preservation,” “alveolar socket preservation (ASP),” and “ARP” are used interchangeably. -
Why do it?
After extraction, the thin cheek-side bone (buccal plate) shrinks first. ARP helps maintain width/contour so later treatment (especially implants) is simpler and less invasive. -
Who is a good candidate?
-
What happens during ARP?
Atraumatic extraction → socket debridement → small amount of graft material placed → socket sealed (collagen membrane or tiny gum graft) → sutures. -
Will it hurt?
Usually similar to a routine extraction. Most patients use standard pain relief for 1–2 days. -
How long is recovery and when can the implant be placed?
Stitches out in ~1–2 weeks; implants commonly at 4–6 months, once the site is stable. (Immediate or early placement is possible in selected cases.) -
What graft materials do you use?
Options include xenograft (e.g., DBBM), human allograft, your own tooth dentin (processed chairside), or synthetics (β-TCP/HA). We pick what best suits your anatomy and preferences. -
Will I still need a graft later?
Sometimes—ARP reduces the amount of shrinkage, so later procedures are smaller and less frequent. -
How much does it cost?
It varies by material and complexity. We provide a written estimate after assessment and CBCT. -
I have an infection—can you still do ARP?
Often yes, after thorough cleaning and decontamination. Severely infected or deficient sockets may be grafted and sealed with a delayed implant plan. -
What if I choose “do nothing”?
Expect more width loss and a higher chance of needing larger grafts (or sinus lift) if you later want an implant. -
What about alternatives like PET (Socket Shield)?
In very select cases and with ideal anatomy/operator skill, PET can further preserve the buccal contour. We’ll discuss if it’s appropriate for you. -
Accordion Title
Accordion content -
Can ARP be combined with an immediate implant?
Yes. If the socket walls are intact and stability is high, we can place an implant and gap-graft around it. If not ideal, ARP with delayed implant is safer. -
What are the risks?
Membrane/seal exposure, infection (uncommon), or residual graft particles on later imaging. Smoking and poor oral hygiene increase risks. Accordion content
Take Away Message
Manage the ridge on day 0. Smart early intervention (ARP or PET where indicated) means fewer flaps, fewer blocks/sinus lifts, and better esthetics later.
Interested in mastering Day-0 ridge management?
Dr Meizi Eliezer offers small-group, hands-on PerioHome courses covering atraumatic extraction, ARP variants (ARP-GM/GS/M/S/G), immediate implant positioning with gap grafting, PET/socket-shield technique, and suturing/soft-tissue seals—plus case selection and CBCT-driven planning. To join the next workshop or arrange in-practice training for your team, contact PerioHome via the site’s contact form, directly on whatsapp or email contact@periohome.co.uk to register your interest.